






我们旨在研究年龄和性别对呼出挥发性有机化合物物质的影响。我们评估了68名健康的成人从不吸烟者,并用年龄和性别。呼气样本通过电子鼻(E-nose)进行分析。导致“呼吸印记”。主成分分析与典型判别分析表明,老年人(≥50岁)不能与年轻的受试者根据他们的呼吸印,以及男性无法与女性区分(交叉验证的准确性,60.3%因此,年龄和性别似乎不会影响整体用电子鼻测量呼出的挥发性有机化合物的分布。
方案详情

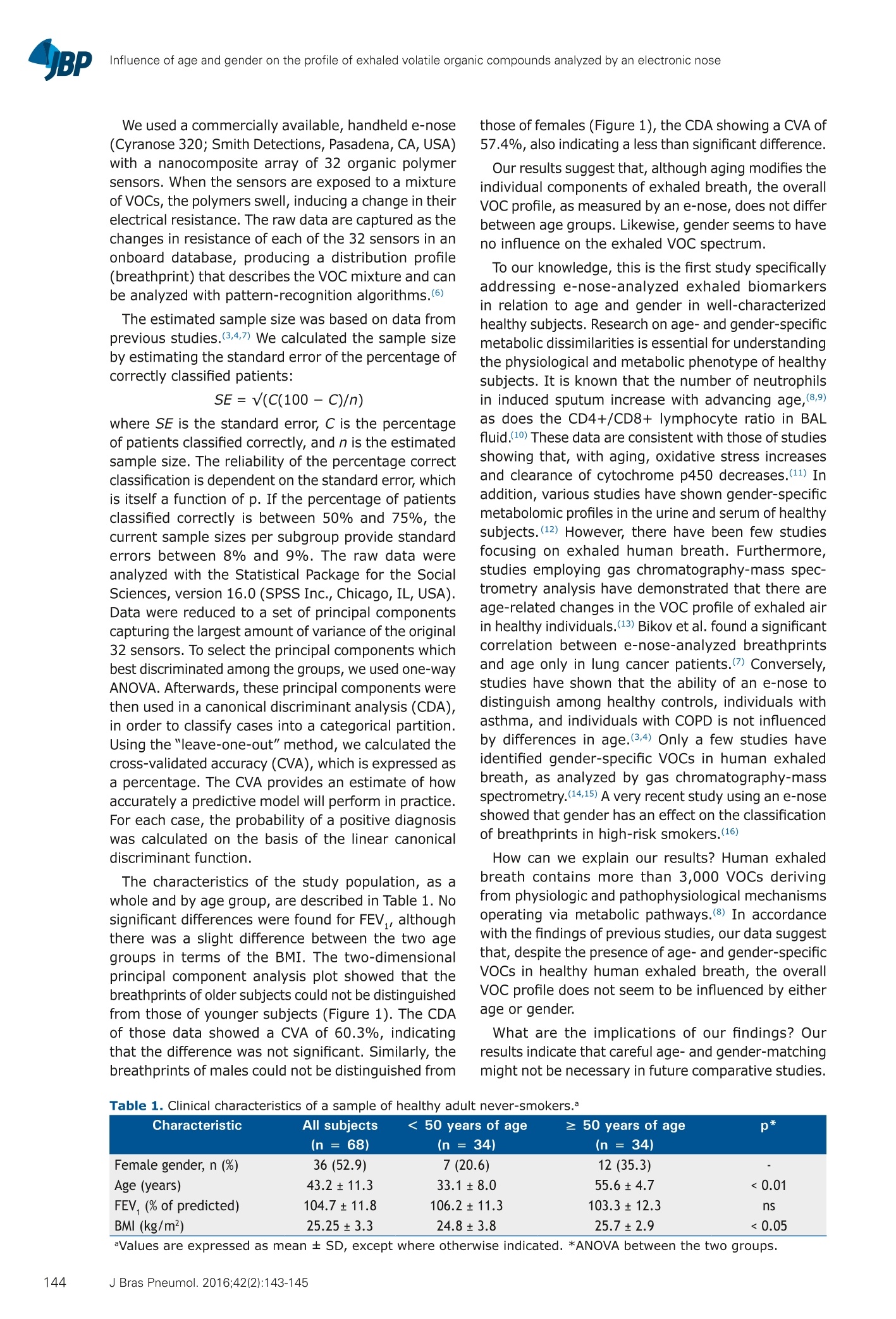
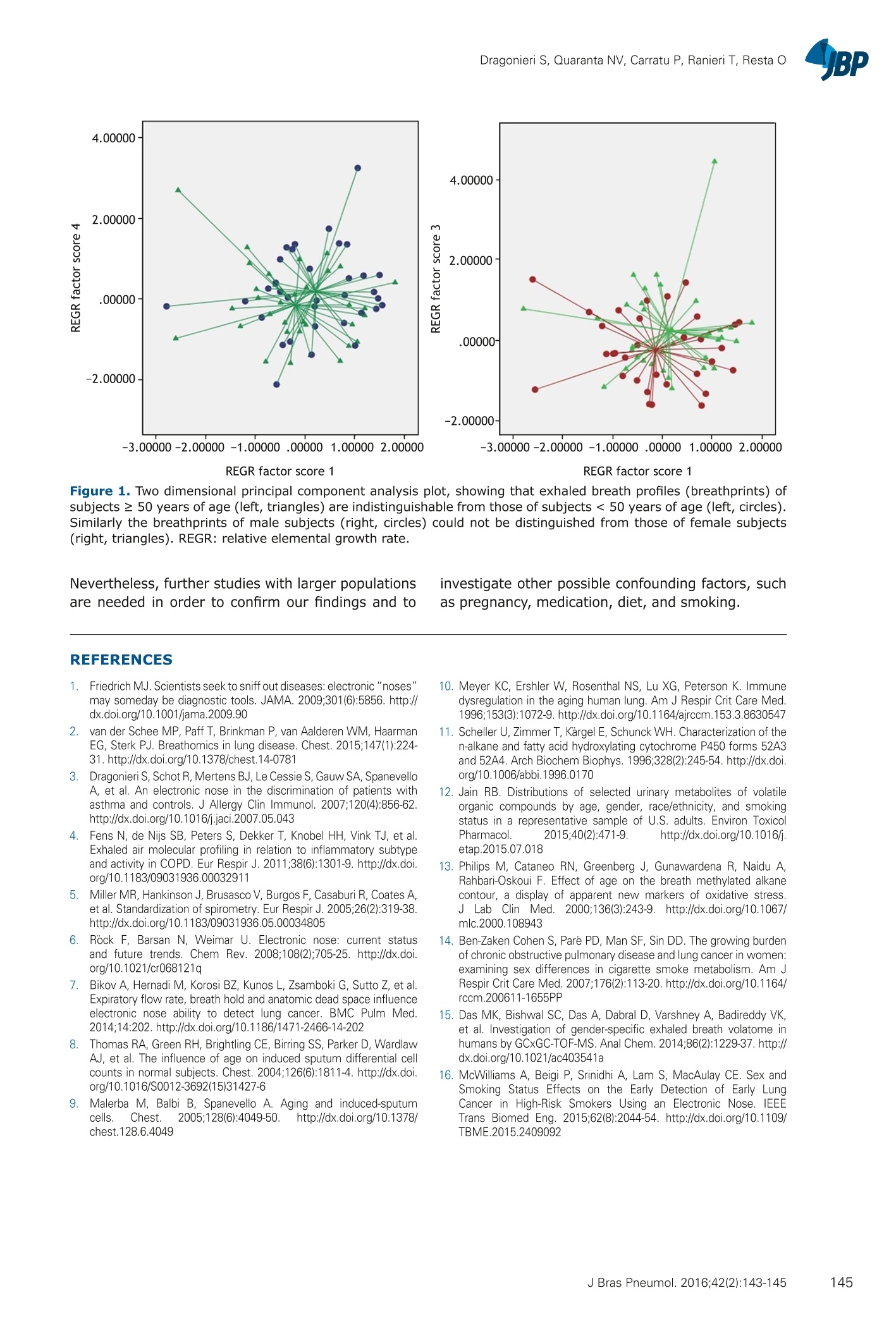
J Bras Pneumol.2016;42(2):143-145BRIEF COMMUNICATIONhttp://dx.doi.org/10.1590/S1806-37562015000000195 Influence of age and gender on the profile of exhaled volatile organic compounds analyzed by an electronic nose 1. Disciplina di Malattie dell'ApparatoRespiratorio, Dipartimento di ScienzeMediche di Base, Neuroscienze eOrgani di Senso, Scuola di Medicina,Universita degli Studi di Bari, Bari, Italia. Submitted: 20 August 2015. Accepted: 30 November 2015. Study carried out in the Disciplina diMalattie dell'Apparato Respiratorio,Dipartimento di Scienze Mediche di Base,Neuroscienze e Organi di Senso, Scuoladi Medicina, Universita degli Studi di Bari,Bari, Italy. Influence of age and gender on the profileof exhaled volatile organic compoundsanalyzed by an electronic nose Silvano Dragonieri1, Vitaliano Nicola Quarantal, Pierluigi Carratul,Teresa Ranieri, Onofrio Restal ABSTRACT We aimed to investigate the effects of age and gender on the profile of exhaled volatileorganic compounds. We evaluated 68 healthy adult never-smokers, comparing them byage and by gender. Exhaled breath samples were analyzed by an electronic nose (e-nose),resulting in "breathprints". Principal component analysis and canonical discriminantanalysis showed that older subjects (≥50 years of age) could not be distinguished fromyounger subjects on the basis of their breathprints, as well as that the breathprints ofmales could not distinguished from those of females (cross-validated accuracy, 60.3%and 57.4%, respectively).Therefore, age and gender do not seem to affect the overallprofile of exhaled volatile organic compounds measured by an e-nose. Keywords: Breath tests; Volatile organic compounds; Electronic nose. Since the discovery of electronic noses, or e-noses, andof their application in the molecular profiling of exhaledbreath (i.e., creation of breathprints), great advanceshave been made with respect to the discrimination ofdiseases through the comparison of overall breathprints.Numerous studies have shown the potential for applyingexhaled volatile organic compound (VOC) profiling in threeclasses of respiratory diseases: lung cancer, respiratoryinfections, and obstructive lung diseases. After the abilityof e-noses to sniff out these diseases was proven, thequestion of what constitutes the exhaled markers ofthose pathologies was raised. Because e-noses assessthe overall mixture of VOCs in exhaled breath, noprimary discriminating markers can be specified as beingsuggestive of the pathophysiological pathways involved.In addition, likely sources of signal interference must beidentified and corrected for, because they are potentiallyconfounding factors.(1) The exhaled VOC profile can beinfluenced by disease-associated factors, such as airwaycaliber and airway inflammation; treatment-associatedfactors, such as medication use; and patient-associatedfactors, such as age, gender, comorbidities, pregnancy,diet, and smoking.(2) Concerning age and gender, thesetwo factors are known to alter VOC levels.(2) Previousstudies on e-nose exhaled breath profiling in severaldiseases have suggested that age does not affect theoverall VOC profile.(3,4) However, to our knowledge, therehave been no studies specifically addressing e-noseanalysis of exhaled biomarkers in relation to age andgender differences in healthy subjects. Therefore, theaim of the present study was to investigate the effectsof age and gender on exhaled breath VOC profiles, asanalyzed by an e-nose,in a population of healthy adults. In this cross-sectional study, exhaled breath sampleswere obtained from 68 healthy adults between 20 and68 years of age. Participants were volunteers recruitedfrom among hospital staff members. We selected anequal number of individuals < 50 years of age (n=34)and ≥ 50 years of age (n = 34). Of the 68 volunteers, 32(47.1%) were male. All were never-smokers, none had ahistory of chest symptoms, and all were free of any knowndisease. All had an FEV,> 70% of the predicted valueand an FEV,/FVC ratio > 80%. None had experienced anyupper or lower respiratory tract infections in the 4 weeksprior to the study. We evaluated the study sample by agegroup (<50 vs. ≥ 50 years of age) and by gender. Thestudy was approved by the Research Ethics Committeeof the University of Bari School of Medicine, in the city ofBari, Italy (Protocol no. 46403/15), and all participatingsubjects gave written informed consent. All measurements were obtained during a single visit.Subjects were asked to refrain from eating and drinking,as well as from engaging in strenuous physical exercise,for at least for 3 h before the visit. Spirometry was performed by a trained lung functiontechnician, in accordance with the latest EuropeanRespiratory Society recommendations,(5) and theequipment (MasterScreen Pneumo; Jaeger; Wurzburg,Germany) was calibrated daily. For all subjects, FEV,and FVC were measured. Exhaled breath analysis wasperformed as previously described.(3) In brief, after 5min of tidal breathing through a3-way non-rebreathingvalve connected to an inspiratory VOC filter (A2; NorthSafety, Middelburg, the Netherlands), subjects exhaled asingle vital capacity volume into a Tedlar bag connectedto an e-nose. ( Correspondence to: ) ( Silvano Dragonieri . D isciplina d i Ma l attie dell'A p parato Respiratorio, D ipartimento di Scienze Me d iche di Bas e , Neuroscienze e Organi di Sen s o, Scuola di Medi c ina, U niversita d e gli S t udi di Bari, Piazza Giulio Cesare, 11, 70 124 , Bari, I talia . ) Tel.: 39 080 559-3215. Email: silvano.dragonieri@uniba.it ( Financial support: None. ) We used a commercially available,handheld e-nose(Cyranose 320; Smith Detections, Pasadena, CA, USA)with a nanocomposite array of 32 organic polymersensors. When the sensors are exposed to a mixtureof VOCs, the polymers swell, inducing a change in theirelectrical resistance. The raw data are captured as thechanges in resistance of each of the 32 sensors in anonboard database, producing a distribution profile(breathprint) that describes the VOC mixture and canbe analyzed with pattern-recognition algorithms.(6) The estimated sample size was based on data fromprevious studies.(3,4,7) We calculated the sample sizeby estimating the standard error of the percentage ofcorrectly classified patients: where SE is the standard error, C is the percentageof patients classified correctly, and n is the estimatedsample size. The reliability of the percentage correctclassification is dependent on the standard error, whichis itself a function of p. If the percentage of patientsclassified correctly is between 50% and 75%, thecurrent sample sizes per subgroup provide standarderrors between 8% and 9%. The raw data wereanalyzed with the Statistical Package for the SocialSciences, version 16.0 (SPSS Inc., Chicago, IL,USA).Data were reduced to a set of principal componentscapturing the largest amount of variance of the original32 sensors. To select the principal components whichbest discriminated among the groups, we used one-wayANOVA. Afterwards, these principal components werethen used in a canonical discriminant analysis (CDA),in order to classify cases into a categorical partition.Using the "leave-one-out"method, we calculated thecross-validated accuracy (CVA), which is expressed asa percentage. The CVA provides an estimate of howaccurately a predictive model will perform in practice.For each case, the probability of a positive diagnosiswas calculated on the basis of the linear canonicaldiscriminant function. The characteristics of the study population, as awhole and by age group, are described in Table 1. Nosignificant differences were found for FEV,,althoughthere was a slight difference between the two agegroups in terms of the BMI. The two-dimensionalprincipal component analysis plot showed that thebreathprints of older subjects could not be distinguishedfrom those of younger subjects (Figure 1).The CDAof those data showed a CVA of 60.3%, indicatingthat the difference was not significant. Similarly, thebreathprints of males could not be distinguished from those of females (Figure 1), the CDA showing a CVA of57.4%, also indicating a less than significant difference. Our results suggest that, although aging modifies theindividual components of exhaled breath, the overallVOC profile, as measured by an e-nose, does not differbetween age groups. Likewise, gender seems to haveno influence on the exhaled VOC spectrum. To our knowledge, this is the first study specificallyaddressing e-nose-analyzed exhaled biomarkersin relation to age and gender in well-characterizedhealthy subjects. Research on age- and gender-specificmetabolic dissimilarities is essential for understandingthe physiological and metabolic phenotype of healthysubjects. It is known that the number of neutrophilsin induced sputum increase with advancing age,(8,9)as does the CD4+/CD8+ lymphocyte ratio in BALfluid.(10) These data are consistent with those of studiesshowing that, with aging, oxidative stress increasesand clearance of cytochrome p450 decreases.(11) Inaddition, various studies have shown gender-specificmetabolomic profiles in the urine and serum of healthysubjects.(12) However, there have been few studiesfocusing on exhaled human breath.Furthermore,studies employing gas chromatography-mass spec-trometry analysis have demonstrated that there areage-related changes in the VOC profile of exhaled airin healthy individuals,(13) Bikov et al. found a significantcorrelation between e-nose-analyzed breathprintsand age only in lung cancer patients.(7) Conversely,studies have shown that the ability of an e-nose todistinguish among healthy controls, individuals withasthma, and individuals with COPD is not influencedby differences in age.(3,4) Only a few studies haveidentified gender-specific VOCs in human exhaledbreath, as analyzed by gas chromatography-massspectrometry.(14,15) A very recent study using an e-noseshowed that gender has an effect on the classificationof breathprints in high-risk smokers.(16) How can we explain our results? Human exhaledbreath contains more than 3,000 VOCs derivingfrom physiologic and pathophysiological mechanismsoperating via metabolic pathways.(8) In accordancewith the findings of previous studies, our data suggestthat, despite the presence of age- and gender-specificVOCs in healthy human exhaled breath, the overallVOC profile does not seem to be influenced by eitherage or gender. What are the implications of our findings? Ourresults indicate that careful age- and gender-matchingmight not be necessary in future comparative studies. Table 1. Clinical characteristics of a sample of healthy adult never-smokers.a Characteristic All subjects < 50 years of age ≥ 50 years of age p* (n = 68) (n = 34) (n = 34) Female gender, n(%) 36(52.9) 7(20.6) 12(35.3) - Age (years) 43.2±11.3 33.1±8.0 55.6±4.7 <0.01 FEV, (% of predicted) 104.7±11.8 106.2±11.3 103.3±12.3 ns BMI (kg/m²) 25.25±3.3 24.8±3.8 25.7±2.9 <0.05 aValues are expressed as mean ± SD, except where otherwise indicated. *ANOVA between the two groups. REGR factor score 1 REGR factor score 1 Figure 1. Two dimensional principal component analysis plot, showing that exhaled breath profiles (breathprints) ofsubjects ≥ 50 years of age (left, triangles) are indistinguishable from those of subjects < 50 years of age (left, circles).Similarly the breathprints of male subjects (right, circles) could not be distinguished from those of female subjects(right, triangles).REGR: relative elemental growth rate. Nevertheless, further studies with larger populationsare needed in order to confirm our findings and to investigate other possible confounding factors, suchas pregnancy, medication, diet, and smoking. REFERENCES ( 1 . Friedrich M J. Scientists s e ek to sniff o ut diseases: electronic" n o s es" may someday be diagnostic tools. JAMA. 200 9 ;301(6):5856. http://dx.doi.org/10.1001/jama.2009.90 ) ( 2. van der Schee MP, P aff T, Brinkman P, va n Aaldere n WM, HaarmanEG, S terk PJ. Breathomics i n lung disease. Chest.2015;147(1):224-31. http://dx.doi.org/10.1378/chest.14-0781 ) ( 3. Dragonieri S, Schot R, Mertens BJ, Le Cessie S, Gauw SA, SpanevelloA, e t a l. An electronic nose in the discrimination of pa t ients withasthma a n d controls. J A l lergy Clin Immunol. 2 0 0 7;120(4):856-62. http://dx.doi.org/10.1016/j.jaci.2007.05.043 ) ( 4 . Fens N, de Nijs S B, Peters S, Dekker T, Knobel H H , Vink TJ , et al. Exhaled air molecular profiling in relatio n to inflammatory subtypeand activity in COPD. E u r R e spir J. 2011;38(6):1301-9. http://dx.doi.org/10 . 1183/09031936.00032911 ) ( 5 . Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A,et al. Standardization of spirometry. Eur Respir J. 20 0 5;26(2):319-38. http://dx.doi.org/10.1183/09031936.05.00034805 ) ( 6. Rock F , B arsan N , W e imar U. El e c tronic nose: cu r rent status and f uture t rends. Chem Re v . 20 0 8;108(2);705-25. http://dx.doi.org/10.1021/cr068121q ) ( 7 . . B iko v A , Hernadi M, Korosi BZ, Kunos L, Zsamboki G, Su t to Z, et al. E xpiratory flow rate, breath hold and anatomic dead space influenceelectronic nose abili t y to dete c t lung canc e r. BM C Pulm Med.2014;14:202. http://dx.doi.org/10.1186/1471-2466-14-202 ) ( 8. Thomas RA, Green RH, Brightling CE, Birring SS, P arker D, Wardlaw AJ, et a l. The i nfluence o f a ge on i n duced sp u tum diff e rential cell counts in n ormal s u bjects. Chest. 2004;126(6):18 1 1-4 . http://dx.doi.org/10.1016/S0012-3692(15)31427-6 ) ( 9. Malerba M , B a lbi B, S panevello A . Aging and induced-sputum cell s . Ches t . 2 : 005;128(6):4049-50. h ttp://dx.doi.org/10. 1 378/ chest.128.6.4049 ) ( 1 0 . Meyer K C, E rshler W, R osenthal N S, L u XG, P eterson K . Immunedysregulation in the aging human lu n g. A m J R e s p ir Crit Care Med . 1 996;153(3):1072-9.ht t p://dx.doi.org/10.1164/ajrccm.153.3.8630547 ) ( 1 1 . Scheller U, Zimmer T, Kargel E, Schunck WH. Characterization of the n -alkane and f atty acid hydroxylating cytochrome P 450 forms 52A3and 52A4. Arch Biochem Biophys. 1996;328(2):245-54.http://dx.doiorg/10.1006/abbi.1996.0170 ) ( 1 2 . Jain R B. D i stributions o f selected ur i nary metabolites of v o la t ileorganic compounds b y age, gender, race/ethnicity, and smokingstatus i n a r epresentative s ample of U.S. adults. E n viron Toxicol Pharmacol. 2 015;40(2):471-9. h ttp://dx.doi.org/10.1016/j. etap.2015.07.018 ) ( 1 3 . Philip s M, Cataneo RN, G reenberg J, G unawardena R, Na i du A,Rahbari-Oskoui F. Effect of age o n the breath me t hylated alk a necontour, a d isplay of apparent n ew m a rkers of ox i dative stress. J La b C li n M e d. 200 0; 136(3):243-9. http : //dx.doi.org/10.1067/ mlc.2000.108943 ) ( 1 4 . Ben-Zaken Cohen S, Pare PD, Man SF, Sin DD. The growing burdenof chronic obstructive pulmonary disease and lung cancer in women: examining sex d i fferences in c igarette smoke m e tabolism. A m J R espir Crit Care Med. 2007;176(2):113 - 20.http://dx.doi.org/10.1164/ rccm.200611-1655PP ) ( 1 5 . Das M K, B i shwal S C , D a s A, D a bral D , V a rshney A, Badireddy VK,et a l. Investigation of gender-specific exhaled breath volatome inhumans by GCxGC-TOF-MS. Anal Chem. 2014;86(2):1229-37.http://dx.doi.org/10.1021/ac403541a ) ( 1 6. McWilliams A , Beigi P, Srinidhi A , La m S, MacAulay CE. Sex and S moking Status E f fects o n t h e Early Detection of Early L ungCancer in H igh-Risk Smokers Using a n E l ectronic Nose. IEEE T rans B iomed En g . 2015;62(8):2044-54 . ht t p://dx.doi.org/10.1 1 09/ T BME.2015.2409092 ) C Sociedade Brasileira de Pneumologia e TisiologiaISSN Bras Pneumol. : 评估了68名健康的成人从不吸烟者,并用年龄和性别。呼气样本通过电子鼻(E-nose)进行分析。导致“呼吸印记”。主成分分析与典型判别分析表明,老年人(≥50岁)不能与年轻的受试者根据他们的呼吸印,以及男性无法与女性区分(交叉验证的准确性,60.3%因此,年龄和性别似乎不会影响整体用电子鼻测量呼出的挥发性有机化合物的分布。
确定

还剩1页未读,是否继续阅读?
产品配置单

图拉扬科技有限公司为您提供《呼出气体中VOCs检测方案(感官智能分析)》,该方案主要用于其他中VOCs检测,参考标准--,《呼出气体中VOCs检测方案(感官智能分析)》用到的仪器有Cyranose 320 电子鼻
推荐专场
感官智能分析系统(电子鼻/电子舌)





相关方案
更多
该厂商其他方案
更多