






方案详情
文
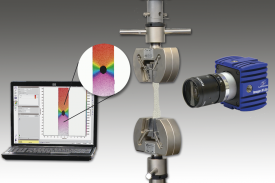
采用Phantom高速相机,用LaVision公司的DaVis软件平台控制图像采集和数据分析,对人咽喉肌肉组织的形态变化进行了记录分析。
方案详情

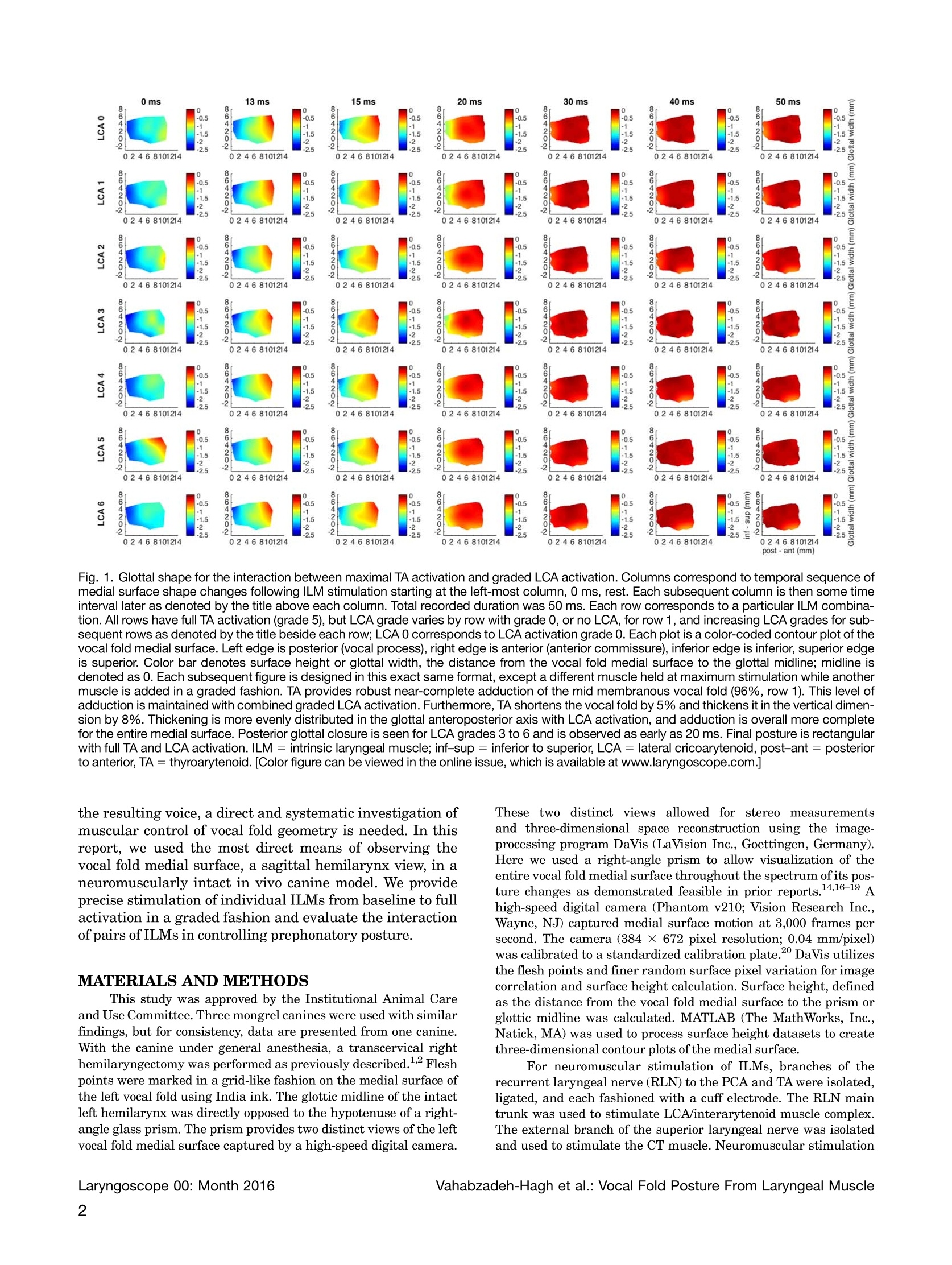
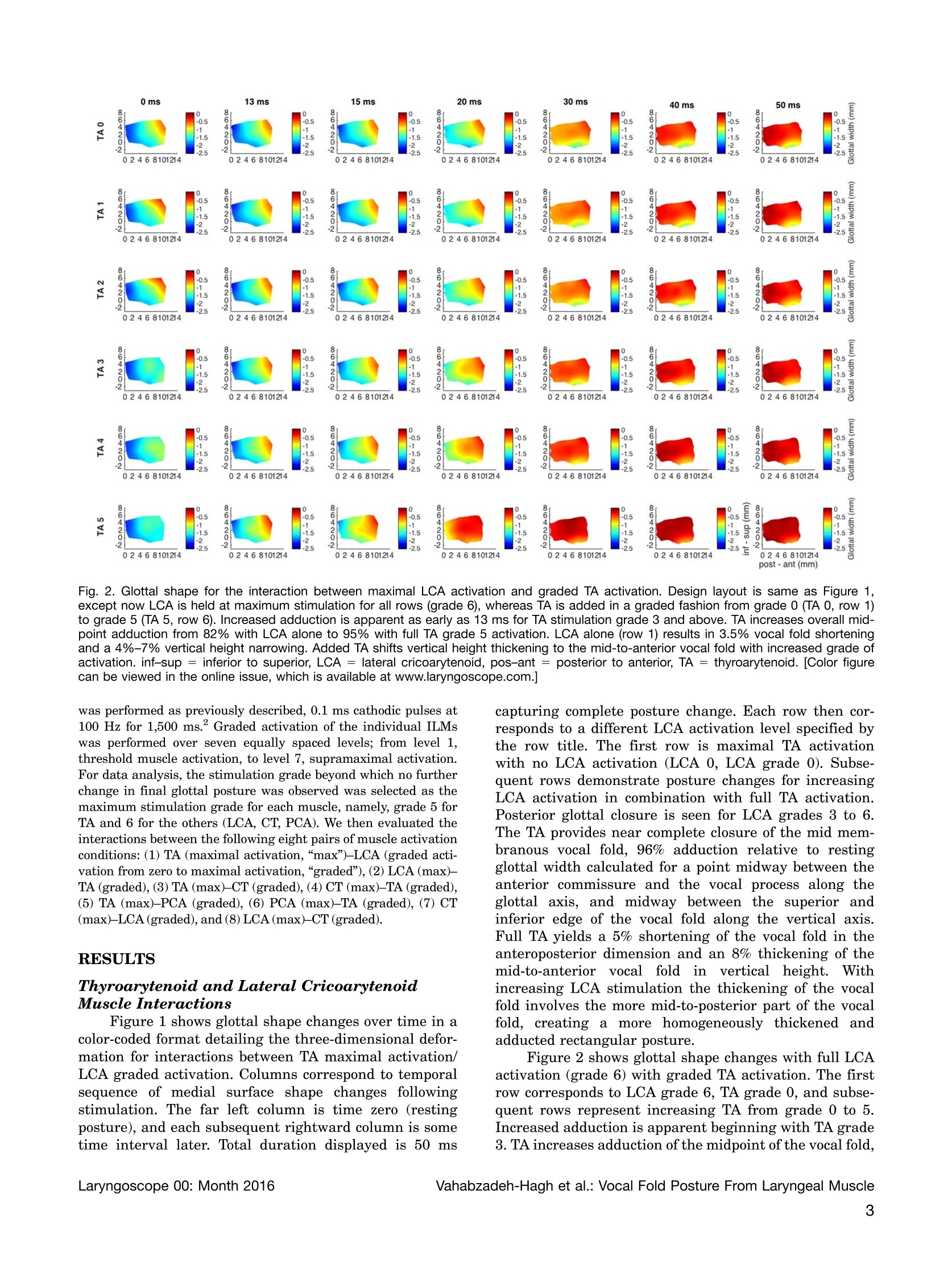
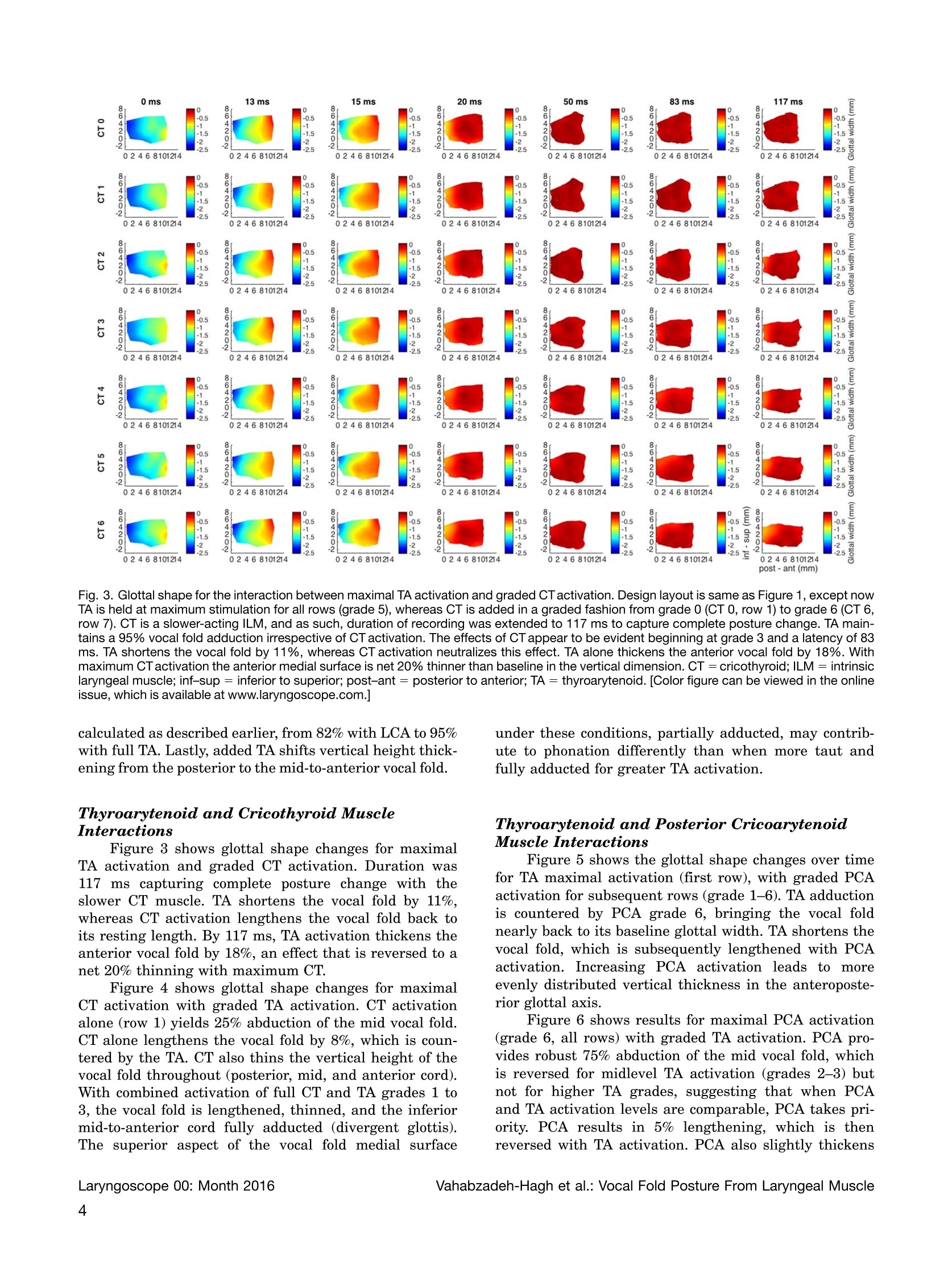
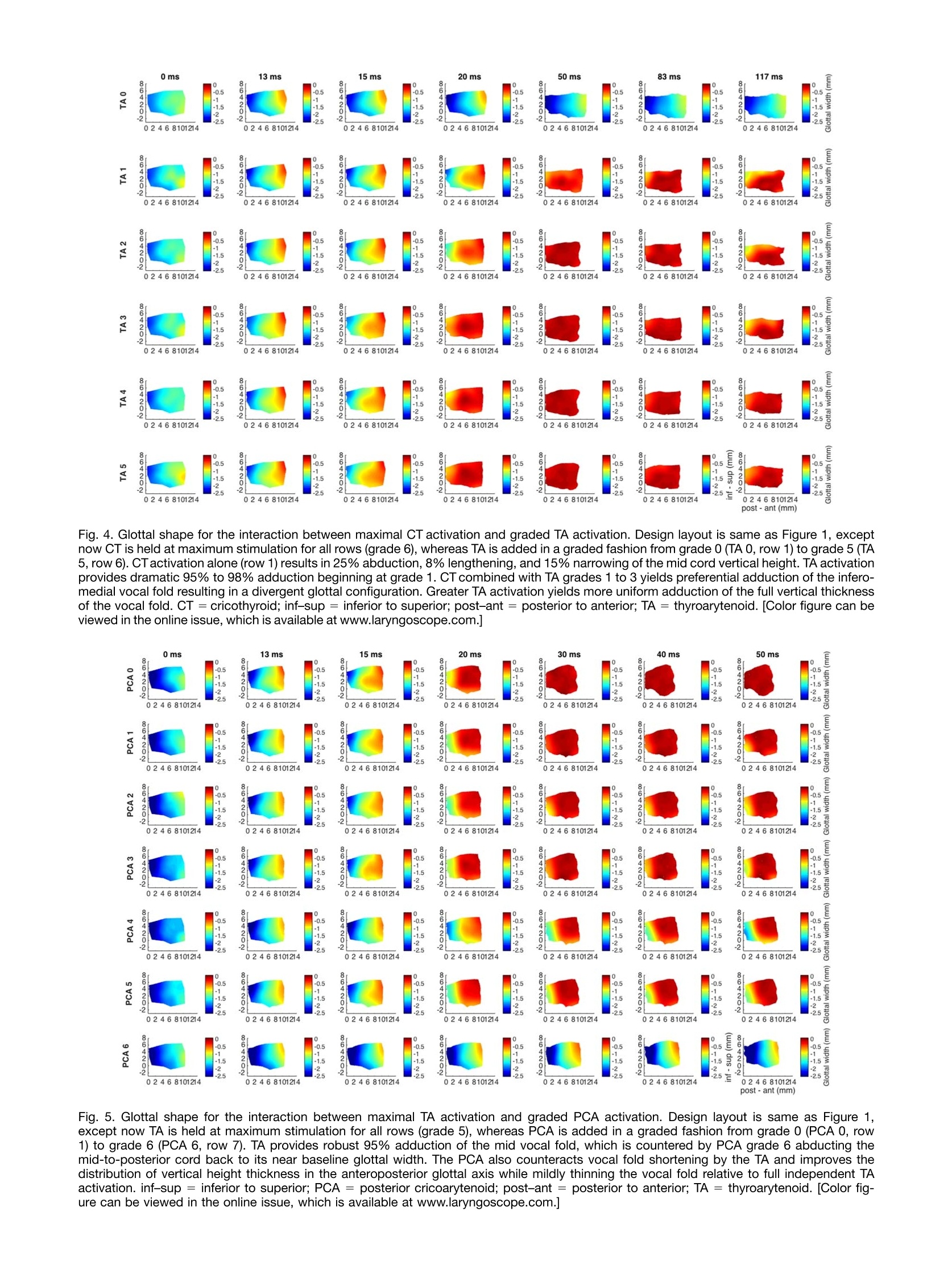
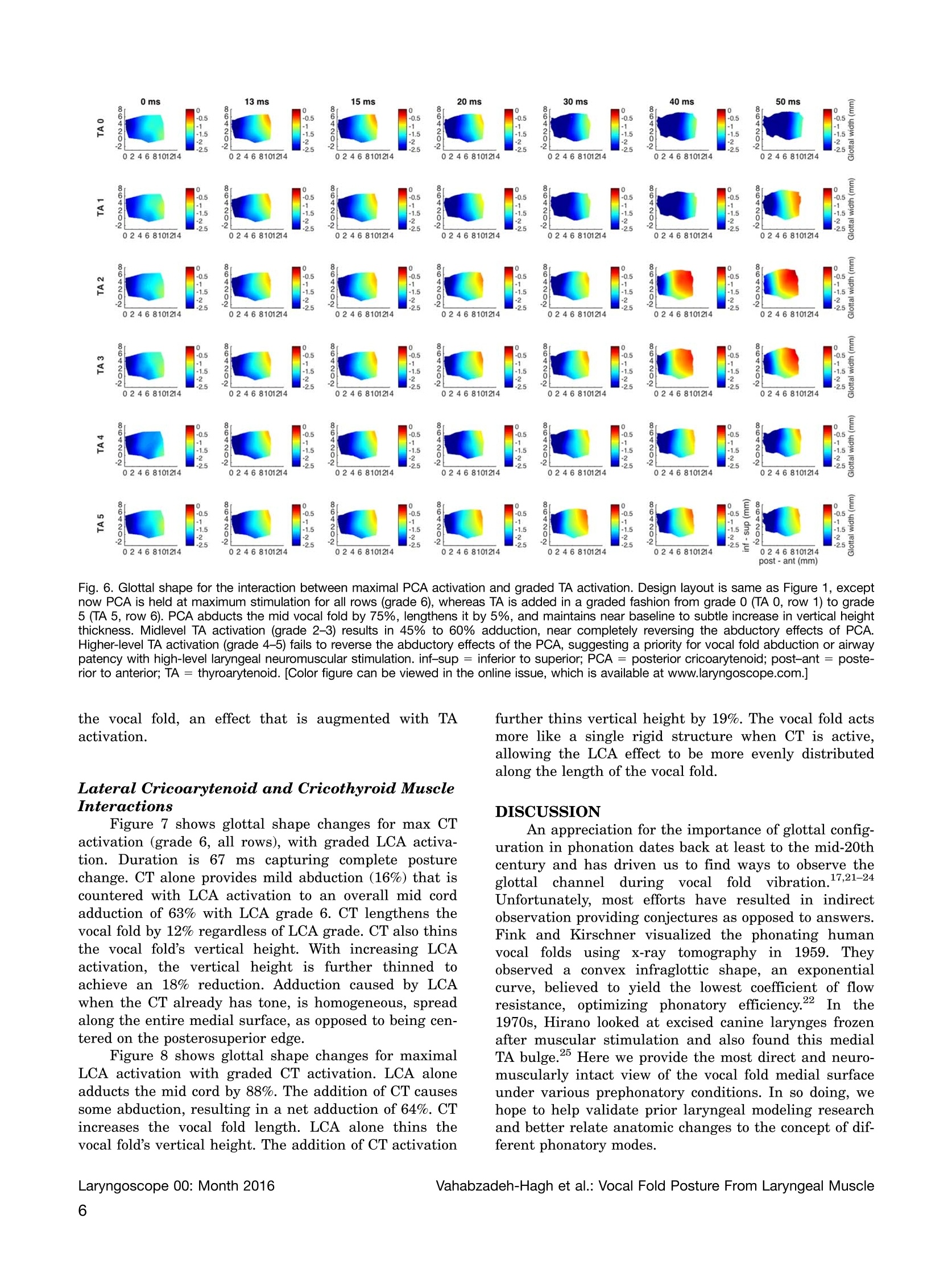
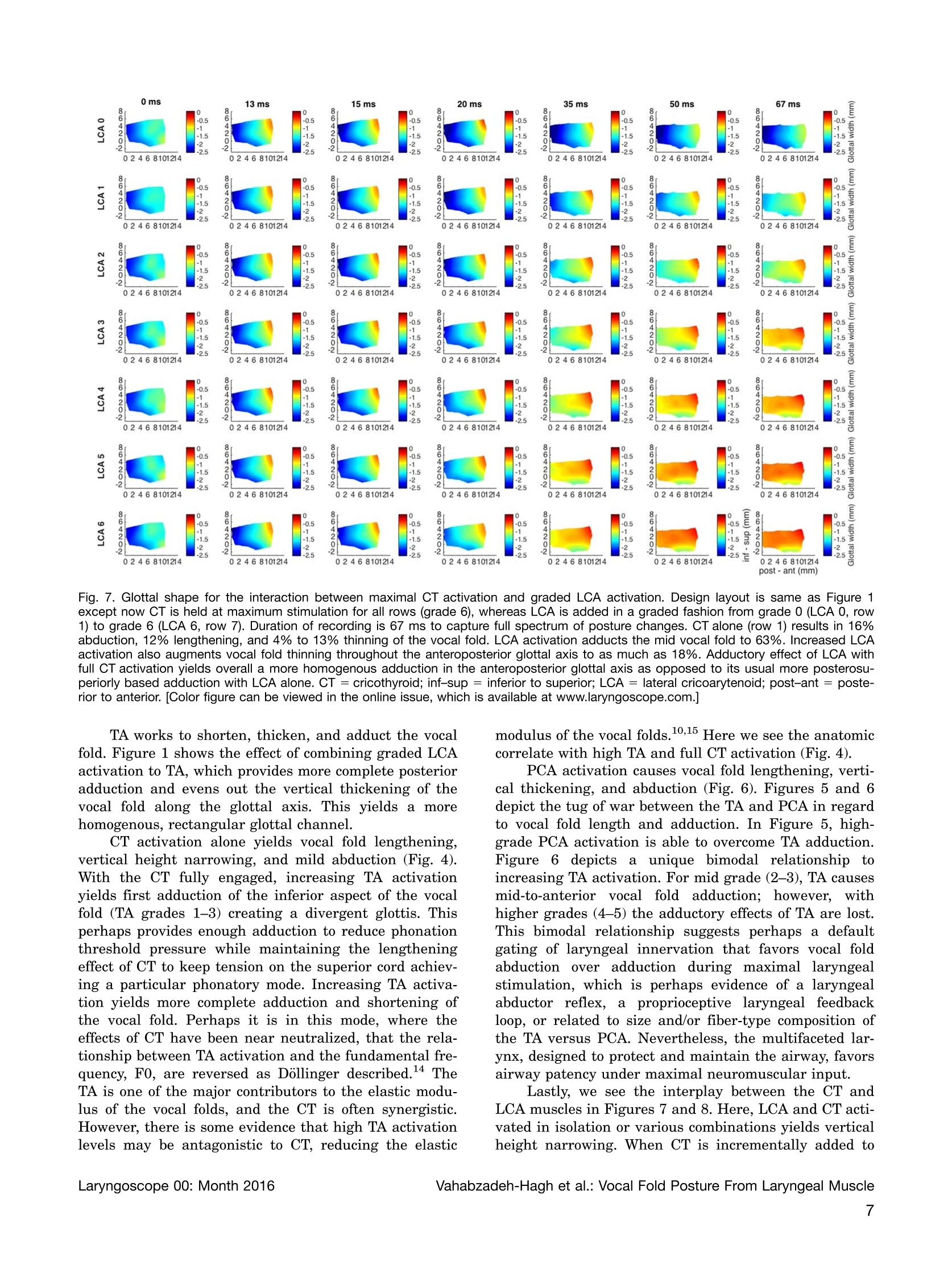
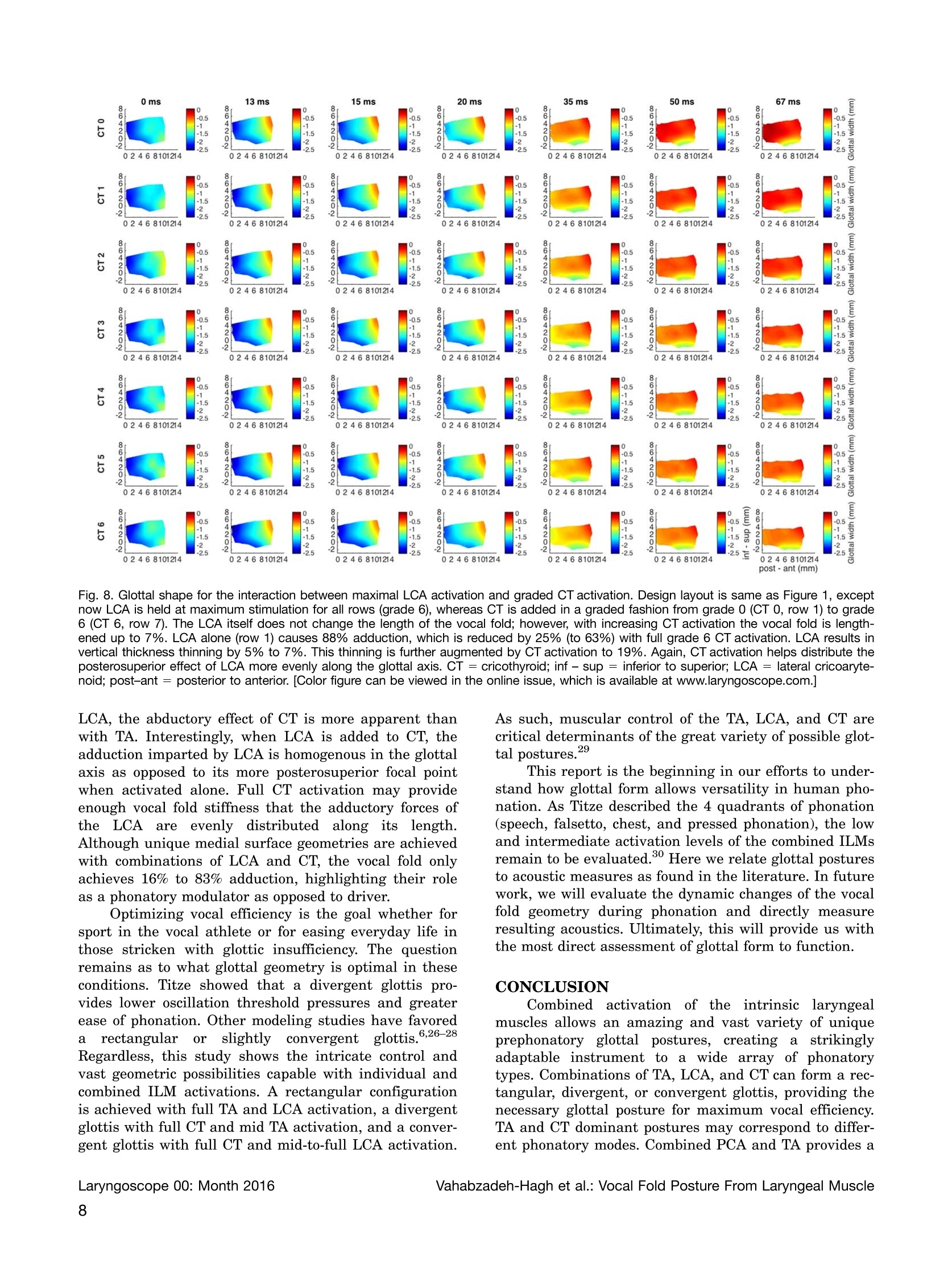
The LaryngoscopeO 2016 The American Laryngological, Three-Dimensional Posture Changes of the Vocal FoldFrom Paired Intrinsic Laryngeal Muscles Andrew M. Vahabzadeh-Hagh,MD; Zhaoyan Zhang, PhD; Dinesh K. Chhetri, MD Objectives/Hypothesis: Although the geometry of the vocal fold medial surface affects voice quality and is critical inthe treatment of glottic insufficiency, the prephonatory shape of the vocal fold medial surface is not well understood. In thisstudy, we activated intrinsic laryngeal muscles individually and in combinations, and recorded the temporal sequence andprecise three-dimensional configurational changes of the vocal fold medial surface. Study Design: In vivo canine hemilarynx model. Methods: A hemilaryngectomy was performed in an in vivo canine model and ink was used to mark the medial surface ofthe in situ vocal fold in a grid-like fashion. The thyroarytenoid (TA), lateral cricoarytenoid (LCA], cricothyroid (CT), and posteriorcricoarytenoid (PCA] muscles were stimulated individually and in combinations. A right-angle prism whose hypotenuse formedthe glottal midline provided two distinct views of the medial surface for a high-speed digital camera. Image-processing packageDaVis (LaVision Inc., Goettingen, Germany) allowed time series cross-correlation analysis for three-dimensional deformation cal-culations of the vocal fold medial surface. Results: Combined TA and LCA activation yields an evenly adducted rectangular glottal surface. Addition of thyroaryte-noid to cricoarytenoid adducts the vocal fold from inferior to superior in a graded fashion allowing formation of a divergentglottis. Posterior cricoarytenoid has a bimodal relationship with thyroarytenoid favoring abduction. Cricothyroid and lateralcricoarytenoid yield unique glottal postures necessary but likely not conducive for efficient phonation. Conclusions: Understanding the three-dimensional geometry of the vocal fold medial surface will help us better under-stand the cause-effect relationship between laryngeal physiology and phonation. Key Words: Larynx, voice, canine, vocal fold, pre-phonatory posture, intrinsic laryngeal muscle. Level of Evidence: NA INTRODUCTION Phonation results from the interaction between aero-dynamic forces acting upon the vocal fold prephonatoryposture. Neuromuscular activation of the intrinsic laryn-geal muscles (ILMs) provides precise control of the vocalfold prephonatory posture, which includes glottal tension,stiffness, and medial surface shape. The vocal fold posturehas a strong influence on the fluid-structure interactionsand resulting vocal fold vibratory mode, phonation type,and the conversion of aerodynamic power to acoustic power.Better understanding muscular control of vocal fold geome-try is thus a critical aspect of better understanding themechanisms of voice production and how geometric modifi-cations of vocal fold contour, such as with injection or type Ithyroplasty, will impact fundamental parameters of voice. ( From the Department o f Head and Neck Surgery, University ofCalifornia Los Angeles, D avid Geffen S c hool o f Medicine, L o s Angeles, California, U.S.A. ) Editor’s Note: This Manuscript was accepted for publication May31,2016. ( Presented a s an o ral presentation at the American Laryngological Association’s 2016 S pring M eeting at C O SM, Chi c ago, Illinois, U. S .A., May 18-19, 2016. ) ( T he a u thors have no oth e r funding, fina n cial rel a tionships, or conflicts of interest to disclose. ) ( Send correspondence to Andrew M. Vahabzadeh-Hagh,MD, 10 8 33 L e C onte Avenue, 62-132, Los Angeles, CA 90095. ) ( E-mail:avahabzadehHagh@mednet.ucla.edu ) ( DOI: 10.1002/lary.26145 ) Glottal channel shape or geometry is primarily orches-trated by four pairs of ILMs: the thyroarytenoid (TA), lat-eral cricoarytenoid (LCA), cricothyroid(CT), and posteriorcricoarytenoid (PCA) muscles.2Optimizing the medialsurface shape has been shown to lower phonation thresholdpressures and improve vocal efficiency. Glottal channelshape, as achieved through differential activation of theILMs, determines voice quality and permits vocal registerand pitch control.-10 Herbst et al. demonstrated fourunique voice qualities resulting from four distinct glottalconfigurations as assessed by videostroboscopy, videoky-nosmography,, andelectroglottography.Kochis-Jenningset al. used electromyography to show TA-dominant phona-tion at lower fundamental frequencies, below 200 to 300Hz, and CT-dominant phonation for chest, head, and fal-setto phonation above 200 to 300 Hz.12,13 Dollinger showedthat TA activation alone achieves chest-like vibrations atlow activation levels and fry-like vibrations with higheractivation.14,15 Understanding how phonatory posture controls voiceproduction and what posture parameters could be manipu-lated with voice therapy or surgery has been limited bylack of quantitative measurements of glottal channel shapewith ILM activation. Specifically, the medial surface of thevocal folds undergoes three-dimensional posture changesthat simply cannot be assessed from the standard two-dimensional endoscopic view. To better understand theinteraction between vocal fold medial surface geometry and Fig. 1. Glottal shape for the interaction between maximal TA activation and graded LCA activation. Columns correspond to temporal sequence ofmedial surface shape changes following ILM stimulation starting at the left-most column, 0 ms, rest. Each subsequent column is then some timeinterval later as denoted by the title above each column. Total recorded duration was 50 ms. Each row corresponds to a particular ILM combina-tion. All rows have full TA activation (grade 5), but LCA grade varies by row with grade 0, or no LCA, for row 1, and increasing LCA grades for sub-sequent rows as denoted by the title beside each row; LCA 0 corresponds to LCA activation grade 0. Each plot is a color-coded contour plot of thevocal fold medial surface. Left edge is posterior (vocal process), right edge is anterior (anterior commissure), inferior edge is inferior, superior edgeis superior. Color bar denotes surface height or glottal width, the distance from the vocal fold medial surface to the glottal midline; midline isdenoted as 0. Each subsequent figure is designed in this exact same format, except a different muscle held at maximum stimulation while anothermuscle is added in a graded fashion. TA provides robust near-complete adduction of the mid membranous vocal fold (96%,row 1). This level ofadduction is maintained with combined graded LCA activation. Furthermore, TA shortens the vocal fold by 5% and thickens it in the vertical dimen-sion by 8%. Thickening is more evenly distributed in the glottal anteroposterior axis with LCA activation, and adduction is overall more completefor the entire medial surface. Posterior glottal closure is seen for LCA grades 3 to 6 and is observed as early as 20 ms. Final posture is rectangularwith full TA and LCA activation. ILM = intrinsic laryngeal muscle; inf-sup=inferior to superior, LCA= lateral cricoarytenoid, post-ant= posteriorto anterior, TA = thyroarytenoid.[Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.] the resulting voice, a direct and systematic investigation ofmuscular control of vocal fold geometry is needed. In thisreport, we used the most direct means of observing thevocal fold medial surface, a sagittal hemilarynx view, in aneuromuscularly intact in vivo canine model. We provideprecise stimulation of individual ILMs from baseline to fullactivation in a graded fashion and evaluate the interactionofpairs ofILMs in controlling prephonatory posture. MATERIALS AND METHODS This study was approved by the Institutional Animal Careand Use Committee. Three mongrel canines were used with similarfindings, but for consistency, data are presented from one canine.With the canine under general anesthesia, a transcervical righthemilaryngectomy was performed as previously described.1.Fleshpoints were marked in a grid-like fashion on the medial surface ofthe left vocal fold using India ink. The glottic midline of the intactleft hemilarynx was directly opposed to the hypotenuse of a right-angle glass prism. The prism provides two distinct views of the leftvocal fold medial surface captured by a high-speed digital camera. These two distinct views allowed for stereo measurementsand three-dimensional space reconstruction using the image-processing program DaVis (LaVision Inc., Goettingen, Germany).Here we used a right-angle prism to allow visualization of theentire vocal fold medial surface throughout the spectrum of its pos-ture changes as demonstrated feasible in prior reports.14,16-19 Ahigh-speed digital camera (Phantom v210; Vision Research Inc.,Wayne, NJ) captured medial surface motion at 3,000 frames persecond. The camera (384 × 672 pixel resolution; 0.04 mm/pixel)was calibrated to a standardized calibration plate.20 DaVis utilizesthe flesh points and finer random surface pixel variation for imagecorrelation and surface height calculation. Surface height, definedas the distance from the vocal fold medial surface to the prism orglottic midline was calculated. MATLAB (The MathWorks, Inc.,Natick, MA) was used to process surface height datasets to createthree-dimensional contour plots of the medial surface. For neuromuscular stimulation of ILMs, branches of therecurrent laryngeal nerve (RLN) to the PCA and TA were isolated,ligated,and each fashioned with a cuff electrode. The RLN maintrunk was used to stimulate LCA/interarytenoid muscle complex.The external branch of the superior laryngeal nerve was isolatedand used to stimulate the CT muscle. Neuromuscular stimulation Fig. 2. Glottal shape for the interaction between maximal LCA activation and graded TA activation. Design layout is same as Figure 1,except now LCA is held at maximum stimulation for all rows (grade 6), whereas TA is added in a graded fashion from grade 0 (TA 0, row 1)to grade 5 (TA 5, row 6). Increased adduction is apparent as early as 13 ms for TA stimulation grade 3 and above. TA increases overall mid-point adduction from 82% with LCA alone to 95% with full TA grade 5 activation. LCA alone (row 1) results in 3.5% vocal fold shorteningand a 4%-7% vertical height narrowing. Added TA shifts vertical height thickening to the mid-to-anterior vocal fold with increased grade ofactivation. inf-sup =inferior to superior, LCA = lateral cricoarytenoid, pos-ant = posterior to anterior, TA = thyroarytenoid. [Color figurecan be viewed in the online issue, which is available at www.laryngoscope.com.] was performed as previously described, 0.1 ms cathodic pulses at100 Hz for 1,500 ms.’Graded activation of the individual ILMswas performed over seven equally spaced levels; from level 1,threshold muscle activation, to level 7, supramaximal activation.For data analysis, the stimulation grade beyond which no furtherchange in final glottal posture was observed was selected as themaximum stimulation grade for each muscle, namely, grade 5 forTA and 6 for the others (LCA, CT, PCA). We then evaluated theinteractions between the following eight pairs of muscle activationconditions: (1) TA (maximal activation,“max")-LCA (graded acti-vation from zero to maximal activation,“graded”),(2) LCA (max)-TA (graded), (3) TA (max)-CT (graded), (4) CT (max)-TA (graded),(5) TA (max)-PCA (graded), (6) PCA (max)-TA (graded), (7) CT(max)-LCA (graded),and(8)LCA (max)-CT (graded). RESULTS Thyroarytenoid and Lateral CricoarytenoidMuscle Interactions Figure 1 shows glottal shape changes over time in acolor-coded format detailing the three-dimensional defor-mation for interactions between TA maximal activation/LCA graded activation. Columns correspond to temporalsequence of medial surface shape changes followingstimulation. The far left column is time zero (restingposture), and each subsequent rightward column is sometime interval later. Total duration displayed is 50 ms capturing complete posture change. Each row then cor-responds to a different LCA activation level specified bythe row title. The first row is maximal TA activationwith no LCA activation (LCA 0, LCA grade 0). Subse-quent rows demonstrate posture changes for increasingLCA activation in combination with full TA activation.Posterior glottal closure is seen for LCA grades 3 to 6.The TA provides near complete closure of the mid mem-branous vocal fold,96% adduction relative to restingglottal width calculated for a point midway between theanterior commissure and the vocal process along theglottal axis, and midway between the superior andinferior edge of the vocal fold along the vertical axis.Full TA yields a 5%shortening of the vocal fold in theanteroposterior dimension and an 8% thickening of themid-to-anterior vocal fold in vertical height. Withincreasing LCA stimulation the thickening of the vocalfold involves the more mid-to-posterior part of the vocalfold, creating a more homogeneously thickened12andadducted rectangular posture. Figure 2 shows glottal shape changes with full LCAactivation (grade 6) with graded TA activation. The firstrow corresponds to LCA grade 6, TA grade 0, and subse-quent rows represent increasing TA from grade 0 to 5.Increased adduction is apparent beginning with TA grade3. TA increases adduction of the midpoint of the vocal fold, Fig. 3.Glottal shape for the interaction between maximal TA activation and graded CT activation. Design layout is same as Figure 1, except nowTA is held at maximum stimulation for all rows (grade 5), whereas CT is added in a graded fashion from grade 0 (CT 0, row 1) to grade 6 (CT 6,row 7). CT is a slower-acting ILM, and as such, duration of recording was extended to 117 ms to capture complete posture change. TA main-tains a 95% vocal fold adduction irrespective of CT activation. The effects of CT appear to be evident beginning at grade 3 and a latency of 83ms. TA shortens the vocal fold by 11%, whereas CT activation neutralizes this effect. TA alone thickens the anterior vocal fold by 18%. Withmaximum CTactivation the anterior medial surface is net 20% thinner than baseline in the vertical dimension. CT = cricothyroid; ILM = intrinsiclaryngeal muscle; inf-sup=inferior to superior; post-ant =posterior to anterior; TA = thyroarytenoid.[Color figure can be viewed in the onlineissue, which is available at www.laryngoscope.com.] calculated as described earlier, from 82% with LCA to 95%with full TA. Lastly, added TA shifts vertical height thick-ening from the posterior to the mid-to-anterior vocal fold. Thyroarytenoid and Cricothyroid MuscleInteractions Figure 3 shows glottal shape changes for maximalTA activation and graded CT activation. Duration was117 ms capturing complete posture change with theslower CT muscle. TA shortens the vocal fold by 11%,whereas CT activation lengthens the vocal fold back toits resting length. By 117 ms, TA activation thickens theanterior vocal fold by 18%, an effect that is reversed to anet 20% thinning with maximum CT. Figure 4 shows glottal shape changes for maximalCT activation with graded TA activation. CT activationalone (row 1) yields 25% abduction of the mid vocal fold.CT alone lengthens the vocal fold by 8%, which is coun-tered by the TA. CT also thins the vertical height of thevocal fold throughout (posterior, mid, and anterior cord).With combined activation of full CT and TA grades 1 to3, the vocal fold is lengthened, thinned, and the inferiormid-to-anterior cord fully adducted (divergent glottis).The superior aspect of the vocal fold medial surface under these conditions, partially adducted,may contrib-ute to phonation differently than when more taut andfully adducted for greater TA activation. Thyroarytenoid and Posterior CricoarytenoidMuscle Interactions Figure 5 shows the glottal shape changes over timefor TA maximal activation (first row), with graded PCAactivation for subsequent rows (grade 1-6). TA adductionis countered by PCA grade 6, bringing the vocal foldnearly back to its baseline glottal width. TA shortens thevocal fold, which is subsequently lengthened with PCAactivation. Increasing PCA activation leads to moreevenly distributed vertical thickness in the anteroposte-rior glottal axis. Figure 6 shows results for maximal PCA activation(grade 6, all rows) with graded TA activation. PCA pro-vides robust 75% abduction of the mid vocal fold, whichis reversed for midlevel TA activation (grades 2-3) butnot for higher TA grades, suggesting that when PCAand TA activation levels are comparable, PCA takes pri-ority. PCA results in 5% lengthening, which is thenreversed with TA activation. PCA also slightly thickens Fig. 4. Glottal shape for the interaction between maximal CT activation and graded TA activation. Design layout is same as Figure 1, exceptnow CT is held at maximum stimulation for all rows (grade 6), whereas TA is added in a graded fashion from grade 0 (TA0, row 1) to grade 5 (TA5, row 6). CTactivation alone (row 1) results in 25% abduction, 8% lengthening, and 15% narrowing of the mid cord vertical height. TA activationprovides dramatic 95% to 98% adduction beginning at grade 1. CT combined with TA grades 1 to 3 yields preferential adduction of the infero-medial vocal fold resulting in a divergent glottal configuration. Greater TA activation yields more uniform adduction of the full vertical thicknessof the vocal fold. CT =cricothyroid; inf-sup = inferior to superior; post-ant = posterior to anterior; TA = thyroarytenoid.[Color figure can beviewed in the online issue, which is available at www.laryngoscope.com.] Fig. 5. Glottal shape for the interaction between maximal TA activation and graded PCA activation. Design layout is same as Figure 1,except now TA is held at maximum stimulation for all rows (grade 5), whereas PCA is added in a graded fashion from grade 0 (PCA 0, row1) to grade 6 (PCA 6, row 7). TA provides robust 95% adduction of the mid vocal fold, which is countered by PCA grade 6 abducting themid-to-posterior cord back to its near baseline glottal width. The PCA also counteracts vocal fold shortening by the TA and improves thedistribution of vertical height thickness in the anteroposterior glottal axis while mildly thinning the vocal fold relative to full independent TAactivation. inf-sup=inferior to superior; PCA = posterior cricoarytenoid; post-ant = posterior to anterior; TA = thyroarytenoid. [Color fig-ure can be viewed in the online issue, which is available at www.laryngoscope.com.] Fig. 6. Glottal shape for the interaction between maximal PCA activation and graded TA activation. Design layout is same as Figure 1, exceptnow PCA is held at maximum stimulation for all rows (grade 6), whereas TA is added in a graded fashion from grade 0 (TA 0, row 1) to grade5 (TA 5, row 6). PCA abducts the mid vocal fold by 75%, lengthens it by 5%, and maintains near baseline to subtle increase in vertical heightthickness. Midlevel TA activation (grade 2-3) results in 45% to 60% adduction, near completely reversing the abductory effects of PCA.Higher-level TA activation (grade 4-5) fails to reverse the abductory effects of the PCA, suggesting a priority for vocal fold abduction or airwaypatency with high-level laryngeal neuromuscular stimulation. inf-sup = inferior to superior; PCA = posterior cricoarytenoid; post-ant =poste-rior to anterior; TA=thyroarytenoid. [Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.] Lateral Cricoarytenoid and Cricothyroid MuscleInteractions Figure 7 shows glottal shape changes for max CTactivation (grade 6, all rows), with graded LCA activa-tion. Duration is 67 ms capturing complete posturechange. CT alone provides mild abduction (16%) that iscountered with LCA activation to an overall mid cordadduction of 63% with LCA grade 6. CT lengthens thevocal fold by 12% regardless of LCA grade. CT also thinsthe vocal fold’s vertical height. With increasing LCAactivation, the vertical height is further thinned toachieve an 18% reduction. Adduction caused by LCAwhen the CT already has tone, is homogeneous, spreadalong the entire medial surface, as opposed to being cen-tered on the posterosuperior edge. Figure 8 shows glottal shape changes for maximalLCA activation with graded CT activation. LCA aloneadducts the mid cord by 88%. The addition of CT causessome abduction, resulting in a net adduction of 64%. CTincreases the vocal fold length. LCA alone thins thevocal fold's vertical height. The addition of CT activation further thins vertical height by 19%. The vocal fold actsmore like a single rigid structure when CT is active,allowing the LCA effect to be more evenly distributedalong the length of the vocal fold. DISCUSSION An appreciation for the importance of glottal config-uration in phonation dates back at least to the mid-20thcentury and has driven us to find ways to observe theglottal channel duringgvocalfoldvibration.17,21-24Unfortunately, most efforts have resulted in indirectobservation providing conjectures as opposed to answers.Fink and Kirschner visualized the phonating humanvocal foldss using x-ray tomography in1959. Theyobserved a convex infraglottic shape, an exponentialcurve, believed to yield the lowest coefficient of flowresistance, optimizing phonatory efficiency.22 In the1970s, Hirano looked at excised canine larynges frozenafter muscular stimulation and also found this medialTA bulge.25 Here we provide the most direct and neuro-muscularly intact view of the vocal fold medial surfaceunder various prephonatory conditions. In so doing, wehope to help validate prior laryngeal modeling researchand better relate anatomic changes to the concept of dif-ferent phonatory modes. Fig. 7. Glottal shape for the interaction between maximal CT activation and graded LCA activation. Design layout is same as Figure 1except now CT is held at maximum stimulation for all rows (grade 6), whereas LCA is added in a graded fashion from grade 0 (LCA 0, row1) to grade 6 (LCA 6, row 7). Duration of recording is 67 ms to capture full spectrum of posture changes. CT alone (row 1) results in 16%abduction, 12% lengthening, and 4% to 13% thinning of the vocal fold. LCA activation adducts the mid vocal fold to 63%. Increased LCAactivation also augments vocal fold thinning throughout the anteroposterior glottal axis to as much as 18%. Adductory effect of LCA withfull CT activation yields overall a more homogenous adduction in the anteroposterior glottal axis as opposed to its usual more posterosu-periorly based adduction with LCA alone. CT = cricothyroid; inf-sup =inferior to superior; LCA= lateral cricoarytenoid; post-ant = poste-rior to anterior. [Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.] TA works to shorten, thicken, and adduct the vocalfold. Figure 1 shows the effect of combining graded LCAactivation to TA, which provides more complete posterioradduction and evens out the vertical thickening of thevocal fold along the glottal axis. This yields a morehomogenous, rectangular glottal channel. CT activation alone yields vocal fold lengthening,vertical height narrowing, and mild abduction (Fig. 4).With the CT fully engaged, increasing TA activationyields first adduction of the inferior aspect of the vocalfold (TA grades 1-3) creating a divergent glottis. Thisperhaps provides enough adduction to reduce phonationthreshold pressure while maintaining the lengtheningeffect of CT to keep tension on the superior cord achiev-ing a particular phonatory mode. Increasing TA activa-tion yields more complete adduction and shortening ofthe vocal fold. Perhaps it is in this mode, where theeffects of CT have been near neutralized, that the rela-tionship between TA activation and the fundamental fre-quency, F0, are reversed as Dollinger described.14 TheTA is one of the major contributors to the elastic modu-lus of the vocal folds, and the CT is often synergistic.However, there is some evidence that high TA activationlevels may be antagonistic to CT, reducing the elastic modulus of the vocal folds. 10,15 Here we see the anatomiccorrelate with high TA and full CT activation (Fig. 4). PCA activation causes vocal fold lengthening, verti-cal thickening, and abduction (Fig. 6). Figures 5 and 6depict the tug of war between the TA and PCA in regardto vocal fold length and adduction. In Figure 5, high-grade PCA activation is able to overcome TA adduction.Figure 6 depicts a unique bimodal relationship) toincreasing TA activation. For mid grade (2-3), TA causesmid-to-anterior vocal fold! adduction; however,withhigher grades (4-5) the adductory effects of TA are lost.This bimodal relationship suggests perhaps a defaultgating of laryngeal innervation that favors vocal foldabduction over adduction during maximallhlaryngealstimulation, which is perhaps evidence of a laryngealabductor reflex, a proprioceptivee laryngeallfeedbackloop, or related to size and/or fiber-type composition ofthe TA versus PCA. Nevertheless, the multifaceted lar-ynx, designed to protect and maintain the airway, favorsairway patency under maximal neuromuscular input. Lastly, we see the interplay between the CT andLCA muscles in Figures 7 and 8. Here, LCA and CT acti-vated in isolation or various combinations yields verticalheight narrowing. When CT is incrementally added to Fig. 8. Glottal shape for the interaction between maximal LCA activation and graded CT activation. Design layout is same as Figure 1, exceptnow LCA is held at maximum stimulation for all rows (grade 6), whereas CT is added in a graded fashion from grade 0 (CT 0, row 1) to grade6 (CT 6, row 7). The LCA itself does not change the length of the vocal fold; however, with increasing CT activation the vocal fold is length-ened up to 7%. LCA alone (row 1) causes 88% adduction, which is reduced by 25% (to 63%) with full grade 6 CT activation. LCA results invertical thickness thinning by 5% to 7%. This thinning is further augmented by CT activation to 19%. Again, CT activation helps distribute theposterosuperior effect of LCA more evenly along the glottal axis. CT = cricothyroid; inf - sup = inferior to superior; LCA = lateral cricoaryte-noid; post-ant = posterior to anterior. [Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.] LCA, the abductory effect of CT is more apparent thanwith TA. Interestingly, when LCA is added to CT, theadduction imparted by LCA is homogenous in the glottalaxis as opposed to its more posterosuperior focal pointwhen activated alone. Full CT activation may provideenough vocal fold stiffness that the adductory forces ofthee LCAare evenly distributedalongitsSlength.Although unique medial surface geometries are achievedwith combinations of LCA and CT, the vocal fold onlyachieves 16% to 83% adduction, highlighting their roleas a phonatory modulator as opposed to driver. Optimizing vocal efficiency is the goal whether forsport in the vocal athlete or for easing everyday life inthose stricken with glottic insufficiency. The questionremains as to what glottal geometry is optimal in theseconditions. Titze showed that a divergent glottis pro-vides lower oscillation threshold pressures and greaterease of phonation. Other modeling studies have favoredarectangular orslightlyy Cconvergent gglottis 6,26-28Regardless, this study shows the intricate control andvast geometric possibilities capable with individual andcombined ILM activations. A rectangular configurationis achieved with full TA and LCA activation, a divergentglottis with full CT and mid TA activation, and a conver-gent glottis with full CT and mid-to-full LCA activation. As such, muscular control of the TA, LCA, and CT arecritical determinants of the great variety of possible glot-tal postures. This report is the beginning in our efforts to under-stand how glottal form allows versatility in human pho-nation. As Titze described the 4 quadrants of phonation(speech, falsetto, chest, and pressed phonation), the lowand intermediate activation levels of the combined ILMsremain to be evaluated.30 Here we relate glottal posturesto acoustic measures as found in the literature. In futurework, we will evaluate the dynamic changes of the vocalfold geometry during phonation and directly measureresulting acoustics. Ultimately, this will provide us withthe most direct assessment of glottal form to function. CONCLUSION Combined1 iactivation of theintrinsiclaryngealmuscles allows an amazing and vast variety of uniqueprephonatory glottala1postures, creatingaa strikinglyadaptable instrument to a wide array of phonatorytypes.Combinations of TA, LCA, and CT can form a rec-tangular, divergent, or convergent glottis, providing thenecessary glottal posture for maximum vocal efficiency.TA and CT dominant postures may correspond to differ-ent phonatory modes. Combined PCA and TA provides a unique bimodal relationship that favors vocal fold abduc-tion. Lastly, CT and LCA yield unique glottal postureslikely necessary but not conducive for efficient phona-tion. Prephonatory posture is the critical substrate forvoice production. Understanding prephonatory posturemay improve our understanding of normal and abnormalvoice production, better guiding our therapeutic efforts. ACKNOWLEDGMENTS This study was supported by grants R01DC011299 andR01DC011300from the National Institutes of Health. BIBLIOGRAPHY 1. Chhetri DK, Neubauer J, Bergeron JL, Sofer E, Peng KA, Jamal N.Effects of asymmetric superior laryngeal nerve stimulation on glotticposture, acoustics, vibration. Laryngoscope 2013;123:3110-3116. 2. Chhetri DK, Neubauer J, Berry DA. Graded activation of the intrinsiclaryngeal muscles for vocal fold posturing. J Acoust Soc Am 2010;127:EL127-EL133 3. Mau T, Muhlestein J, Callahan S, Chan RW. Modulating phonationthrough alteration of vocal fold medial surface contour. Laryngoscope2012;122:2005-2014. 4. Scherer RC, Shinwari D, De Witt KJ, Zhang C, Kucinschi BR, Afjeh AA.Intraglottal pressure profiles for a symmetric and oblique glottis with adivergence angle of 10 degrees. J Acoust Soc Am 2001;109:1616-1630. 5. Scherer RC, Shinwari D, De Witt KJ, Zhang C, Kucinschi BR, Afjeh AA.Intraglottal pressure distributions for a symmetric and oblique glottis?00?.11?.with a uniform duct. J Acoust Soc Am 2002;112:1253-1256. 6. Titze IR. The physics of small-amplitude oscillation of the vocal foldsJ Acoust Soc Am 1988;83:1536-1552. 7. Courey MS. Homologous collagen substances for vocal fold augmentationLaryngoscope 2001;111:747-758. .8. Titze IR. A framework for the study of vocal registers. J Voice 1988;23:1-12.9).. Vilkman E, Alku P,Laukkanen AM. Vocal-fold collision mass as a differen- tiator between registers in the low-pitch range. J Voice 1995;9:66-73. 10. Zhang Z. Cause-effect relationship between vocal fold physiology and voiceproduction in a three-dimensional phonation model. J Acoust Soc Am.2016;139(4):1493. 11. Herbst CT, Ternstrom S, Svec JG. Investigation of four distinct glottal con-figurations in classical singing-a pilot study. J Acoust Soc Am 2009;125:EL104-EL109. 12. Kochis-Jennings KA, Finnegan EM, Hoffman HT, Jaiswal S. Laryngealshfmuscle activity and vocal fold adduction during chest, chestmix, head-mix,and head registers in females. J Voice 2012;26:182-193. . 13. Kochis-Jennings KA, Finnegan EM, Hoffman HT, Jaiswal S, Hull D. Cri-cothyroid muscle and thyroarytenoid muscle dominance in vocal registercontrol: preliminary results. J Voice 2014;28:652.e621-652.e629. 14. Dollinger M, Berry DA, Berke GS. Medial surface dynamics of an in vivo . canine vocal fold during phonation.J Acoust Soc Am 2005;117:3174-3183.15. Berke GS, Gerratt BR. Laryngeal biomechanics: an overview of mucosalwave mechanics. J Voice 1993;7:123-128. 16. Abdel-Aziz Y, Karara H. Direct linear transformation from comparatorcoordinates into objec9st space coordinates in close-range photogrammetry.Proceedings of the ASP/UI Symposium on Close-Range Photogrammetry,Urbana, Illinois. 1971:1-18. 17. Berry DA, Montequin DW, Tayama N. High-speed digital imaging of themedial surface of the vocal folds. J Acoust Soc Am 2001;110(5 pt 1)2539-2547. 18. Chen L, Armstrong CW, Raftopoulos DD. An investigation on the accuracy: of three-dimensional space reconstruction using the direct linear trans-formation technique. J Biomech 1994;27:493-500. 19. Doellinger M, Berry DA, Berke GS. A quantitative study of the medialsurface dynamics of an in vivo canine vocal fold during phonationLaryngoscope 2005;115:1646-1654. 20. Zhang Z, Neubauer J, Berry DA. Aerodynamically and acoustically drivenmodes of vibration in a physical model of the vocal folds. J Acoust SocAm 2006;120(5 pt 1):2841-2849. 21. Farnsworth D. High-speed motion pictures of the human vocal cords. BellLab 1940;Rec 18:203-208. 22. Fink BR, Kirschner F. Observations on the acoustical and mechanicalproperties of the vocal folds. Folia Phoniatr (Basel) 1959;11:167-172. 23. Hess MM, Ludwigs M. Strobophotoglottographic transillumination as amethod for the analysis of vocal fold vibration patterns. J Voice 2000;14:255-271. 24. Saito S, Fukuda H, Isohai Y, Ono H. X-ray stroboscopy. In: Stevens K, ed Vocal Fold Physiology. Tokyo, Japan: University of Tokyo; 1981:95-106.25. Hirano M. Vocal mechanisms in singing: laryngological and phoniatricaspects.J Voice 1988;2:51-69. 26. Chan RW, Titze IR, Titze MR. Further studies of phonation thresholdpressure in a physical model of the vocal fold mucosa. J Acoust Soc Am1997;101:3722-3727. 27. Lucero JC. Optimal glottal configuration for ease of phonation.J Voice1998;12:151-158 28. Zhang Z. Influence of flow separation location on phonation onsetJ Acoust Soc Am 2008;124:1689-1694. 29. Chhetri DK,Neubauer J. Differential roles for the thyroarytenoid and lateralcricoarytenoid muscles in phonation. Laryngoscope 2015;125:2772-2777. 30. Titze IR. Principles of Voice Production. Iowa City, IA: National Center forVoice and Speech; 2000:281-303. Vahabzadeh-Hagh et al.: Vocal Fold Posture From Laryngeal MuscleLaryngoscope Month Phonation results from the interaction between aerodynamicforces acting upon the vocal fold prephonatoryposture. Neuromuscular activation of the intrinsic laryngealmuscles (ILMs) provides precise control of the vocalfold prephonatory posture, which includes glottal tension,stiffness, and medial surface shape. The vocal fold posturehas a strong influence on the fluid-structure interactionsand resulting vocal fold vibratory mode, phonation type,and the conversion of aerodynamic power to acoustic power.Better understanding muscular control of vocal fold geometryis thus a critical aspect of better understanding themechanisms of voice production and how geometric modificationsof vocal fold contour, such as with injection or type Ithyroplasty, will impact fundamental parameters of voice.
确定


还剩7页未读,是否继续阅读?
产品配置单


北京欧兰科技发展有限公司为您提供《配对喉内肌中观察声带的三维姿态变化检测方案(其它无损检测仪器/设备)》,该方案主要用于其他中观察声带的三维姿态变化检测,参考标准--,《配对喉内肌中观察声带的三维姿态变化检测方案(其它无损检测仪器/设备)》用到的仪器有LaVision StrainMaster材料应变形变成像测量系统、LaVision HighSpeedStar 高帧频相机
推荐专场




相关方案
更多
该厂商其他方案
更多